Bioquark Inc. (www.bioquark.com) Interview in MoneyWeek
Read whole story: http://moneyweek.com/who-wants-to-live-forever/

Bioquark Inc. (www.bioquark.com) Interview in MoneyWeek
Read whole story: http://moneyweek.com/who-wants-to-live-forever/


Bioquark, Inc., (http://www.bioquark.com) a life sciences company focused on the development of novel, natural bio-products for health, wellness and rejuvenation, has entered a collaboration whereby Forest Organics LLC & I-Beauty Charm LLC, a unique, integrated facial and body cosmetology facility, and their state-licensed, highly skilled skin care specialists, will be utilizing novel, natural Bioquantine™ extract complexes as part of their spa procedures, as well as providing consumer access to a range of proprietary skin care products (http://www.forestorganics.life).
“We are very excited about this first company collaboration in the area of beauty care and cosmetology,” said Ira S. Pastor, CEO, Bioquark Inc. “It is another step forward towards the wide applicability of our natural combinatorial bio-products, across a broad range of health and wellness segments, as well as future franchise opportunities.”
The integrated Forest Organics LLC & I-Beauty Charm LLC model was conceived by local Tampa business women, Nadia Goetzinger and Tatyana Reshetnikova, to offer a new generation of products and services related to skin beautification and rejuvenation.
“We look forward to working closely with Bioquark Inc. on this initiative and providing an exclusive range of services and products to customers throughout the greater Tampa metropolitan area,” said Ms. Goetzinger”
About Bioquark, Inc.
Bioquark Inc. is focused on the development of natural biologic based products, services, and technologies, with the goal of curing a wide range of diseases, as well as effecting complex regeneration. Bioquark is developing both biopharmaceutical candidates, as well as non-Rx products for the global consumer health and wellness market segments.
About Forest Organics LLC & I-Beauty Charm LLC
Forest Organics LLC & I-Beauty Charm LLC operate a unique, integrated facial and body cosmetology facility providing novel rejuvenative spa and cosmetology services and products.

Philadelphia, PA, USA / Mexico City, Mexico — Bioquark, Inc., (www.bioquark.com) a life sciences company focused on the development of novel bioproducts for complex regeneration, disease reversion, and aging, and RegenerAge SAPI de CV, (www.regenerage.clinic/en/) a clinical company focused on translational therapeutic applications of a range of regenerative and rejuvenation healthcare interventions, have announced a collaboration to focus on novel combinatorial approaches in human disease and wellness. SGR-Especializada (http://www.sgr-especializada.com/), regulatory experts in the Latin American healthcare market, assisted in the relationship.
“We are very excited about this collaboration with RegenerAge SAPI de CV,” said Ira S. Pastor, CEO, Bioquark Inc. “The natural synergy of our cellular and biologic to applications of regenerative and rejuvenative medicine will make for novel and transformational opportunities in a range of degenerative disorders.”
As we close in on $7 trillion in total annual health care expenditures around the globe ($1 trillion spent on pharmaceutical products; $200 billion on new R&D), we are simultaneously witnessing a paradoxical rise in the prevalence of all chronic degenerative diseases responsible for human suffering and death.
With the emergence of such trends including: personalization of medicine on an “n-of-1” basis, adaptive clinical design, globalization of health care training, compassionate use legislative initiatives for experimental therapies, wider acceptance of complementary medical technologies, and the growth of international medical travel, patients and clinicians are more than ever before, exploring the ability to access the therapies of tomorrow, today.
The estimate of the current market size for procedural medical travel, defined by medical travelers who travel across international borders for the purpose of receiving medical care, is in the range of US $40–55 billion.
Additionally, major clinical trial gaps currently exist across all therapeutic segments that are responsible for human suffering and death. Cancer is one prime example. As a leading cause of morbidity and mortality worldwide for many decades, today there are approximately 14 million new cases diagnosed each year, with over 8 million cancer related deaths annually. It is estimated that less than 5% of these patients, take the initiative to participate in any available clinical studies.
“We look forward to working closely with Bioquark Inc. on this exciting initiative,” said Dr. Joel Osorio, Chief of Clinical Development RegenerAge SAPI de CV. “The ability to merge cellular and biologic approaches represents the next step in achieving comprehensive regeneration and disease reversion events in a range of chronic diseases responsible for human suffering and death.”
About Bioquark, Inc.
Bioquark Inc. is focused on the development of natural biologic based products, services, and technologies, with the goal of curing a wide range of diseases, as well as effecting complex regeneration. Bioquark is developing both biological pharmaceutical candidates, as well as products for the global consumer health and wellness market segments.
About RegenerAge SAPI de CV
RegenerAge SAPI de CV is a novel clinical company focused on translational therapeutic applications, as well as expedited, experimental access for “no option” patients, to a novel range of regenerative and reparative biomedical products and services, with the goal of reducing human degeneration, suffering, and death.
Philosophers have been debating the meaning of life for millennia. Billions of people believe that the principal aim in life is to experience pleasure, and they try to enjoy life as much as possible before they die. A minority of others, make it their life’s aim to achieve something which is over and above simple pleasure: not merely to help others, not even to help humanity at large. They aim, whether knowingly or unknowingly, to improve the evolutionary process of nature as a whole.
So far, so good. But it appears that the view we hold about our life, our worldview, has a direct impact on our biology. We know that thinking positively may help improve the immune system. But research also shows that people who aim for pleasure (Hedonia) may have an impaired genetic profile, compared to those who aim for higher virtues (Eudaimonia). There is a distinction between these two terms and it is worth providing a definition here:
Hedonia is an exclusive search for pleasure and avoidance of discomfort. It may involve increased emphasis on eating well, drinking, dancing, playing, and generally enjoying simple pleasures in life. It is contentment, gratification, fun, merriment, satisfaction and, perhaps necessarily, a lack of motivation to search for a nobler aim in life. One may argue that hedonia involves a risk that leads to bad health due to a tendency to excesses (smoking, alcohol, coffee, sweets), a general inclination to avoid uncomfortable physical activity, and a lack of challenging cognitive effort. The risk of addiction may be increased. Erosion of social bonds become a possibility when a hedonist is more concerned about his/her own pleasure and is less sensitive to the needs of others.
Eudaimonia is a term reflecting the highest ‘intellectual good’. It is virtue plus excellence, superior ethical refinement, cognitive sophistication, as well as other qualities such as persistent motivation, wisdom, imagination, creativity, vision and a feeling of purpose. The term has been discussed by many ancient Greek philosophers particularly Aristotle and the Stoics. In modern times and in a wider sense, eudaimonia may be equated with meaningful technological hyperconnection, or ‘Intentional Evolution’, an attempt to constructively improve the human condition in all respects (including those relating to the wider universe). Hedonia is found both in animals and in humans, whereas eudaimonia is only found in humans.
The above descriptions deliberately avoid the mention of the term ‘happiness’. People may fulfil either hedonic or eudaimonic characteristics and still be happy or unhappy nevertheless. Although hedonia and eudaimonia are distinct concepts, both are philosophical notions of happiness.
It has been suggested that eudaimonic well-being is associated with increased volume of a specific part of our brain, the right insular cortex although it is not known if this increase is the cause or the result of eudaimonia. The insula has been implicated in higher abstract functions such as self-awareness, self-reflection, cognitive control and intentional, creative goal-directed behaviour.
Eudaimonia is influenced by genetic factors and not so much by the environment. In a classic paper, high eudaimonic well-being was associated with a decreased risk of depression, improved physical health, improved sleep patterns, a reduction of inflammation and stress markers, together with a lower risk of cardiovascular disease. By contrast, high hedonic well-being was not associated with any of these.
We know that the immune system may have an impact on social behaviour. In a study published yesterday, scientists have shown that a component of the immune system, namely interferon-γ, can control neuronal connectivity in areas of the brain which are implicated in social interactions. This is the new science of Social Genomics, which may help us understand the mechanisms involved in the interaction between our social and emotional self and our biology. Social Genomics study the influence of social factors such as loneliness, stress, conflict, cooperation, and interaction with technology, upon our genetic profile and gene expression. Scientists in social genomics have analysed gene expression in the white blood cells of healthy adults, and showed that those who fulfilled the hedonic criteria exhibited a higher expression of stress-related and inflammation-increasing factors. We know that stress and inflammation are implicated in ageing. In contrast, those people who fulfilled primarily the eudaimonic characteristics showed the opposite genetic features, namely a down-regulation of inflammatory markers and an improvement of certain immune factors. These findings were confirmed again. Although both hedonia and eudaimonia may contribute to a feeling of subjective well-being, it appears that eudaimonia is associated with a measurable health effect which is defined by objective genetic and biological characteristics.
This begs the question: Does ageing and early death have something to do with hedonism? And at the same time, is the pursuit of eudaimonia one of the prerequisites for long, healthy life? I addressed this issue from different perspectives in a blog and a paper. Over the past years I have argued that being meaningfully hyperconnected and searching for a nobler aim in life are characteristics associated with longevity (because such characteristics increase the information content of the individual and may improve cellular repair – the Indispensable Soma hypothesis).
Evolution tends to follow a trajectory defined by survival and, in the case of humans, it is biased towards achieving a higher common good, a stage which is better than the previous one. If this is the case, there should be conserved signalling pathways and other biological mechanisms which favour a continuation of survival AND the ability to contribute to the universal good. Merely seeking pleasure is seen, from an evolutionary perspective, as just surviving without the need to achieve anything higher. Thus, hedonia appears to be in conflict with the basic trajectory of evolution. In addition, there is another puzzling question: Why is eudaimonia found only in humans and not in other animals? If eudaimonia is a pathway that leads to an improvement in the human condition we may need to espouse it fully, in order to improve ourselves and achieve longer life as a result. In fact, it could be the ONLY path towards achieving extreme longevity. Waiting for others to come up with pills and treatments to ‘cure’ ageing, is just…hedonic, it reflects an avoidance of effort and unwillingness to deal with the matter ourselves.
So, here is a concept for debate: People who live within a cognitive ecosystem and actively pursue eudaimonic characteristics are likely to enjoy better health, and have increased chances of living longer, compared to those who merely seek personal pleasure. This makes sense from clinical, biological, evolutionary and philosophical standpoints.
Its painful to bear views that make many think I’m an imbicile and dislike me. So please, if anybody has a rational argument why any of this is wrong, I beg to be enlightened. I’ve set up a diagram for the purpose that will support you to add your criticism exactly where it is pertinent. https://truthsift.com/graph/Are-Vaccines-Safe/406/0/-1/-1/0/0/0/0/0/0/0/0/0/0/0/0/0/0/0/0
(1) The National Academy’s Reviews Of Vaccine Safety
The Institute of Medicine of the National Academies has provided several multi-hundred page surveys studying the safety of vaccines, but rather than reassuring, these itemize some iatrogenic conditions being caused, and pronounce the scientific literature inadequate to say whether most others are. The 2011 Institute of Medicine (IOM) Review[1] looked at 146 vaccine-condition pairs for causality, reporting:
The 2003 IOM Review on multiple vaccines said[2]:
“The committee was unable to address the concern that repeated exposure of a susceptible child to multiple immunizations over the developmental period may also produce atypical or non-specific immune or nervous system injury that could lead to severe disability or death (Fisher, 2001). There are no epidemiological studies that address this.”
and:
“the committee concludes that the epidemiological and clinical evidence is inadequate to accept or reject a causal relationship between multiple immunization and an increased risk of allergic disease, particularly asthma.”
(2) The Aluminum.
Alum was added to vaccines back in the 1920’s, with no test of parenteral toxicity until recently[5], because it prods the immature immune system out of its normal operating range.[6] Maybe they figured aluminum is common in the environment, but injection bypasses half a dozen evolved sequential filters that normally keep it out of circulatory flow during development. Vaccines put hundreds of times as much aluminum into infants’ blood as they would otherwise get, and in an unnatural form that is hard for the body to remove.[7][8 (cfsec 4.2)][9]. The published empirical results indicate its highly toxic.
(3) The Safety Studies Ignore Confounding Patient Behavior
Since there are no Randomized Placebo Controlled (RPC) trials supporting vaccines, virtually all studies report on the association (or lack thereof) between vaccines and some iatrogenic condition. But parents who believe vaccines made their kids sick, stop vaccinating them, which systematically moves sick or vaccine damaged kids in the studies into the “low vaccine”, “low thimerisol”, or etc. bin. This invalidates most studies supporting safety (and the few remaining ones suck for other reasons). Numerous studies report incredible preventative effects for vaccines, presumably because of this corruption, like having more thimerisol or more MMR’s is strongly preventative of autism and other mental development issues[28][29][30], or like having more vaccines was strongly preventative of atopy, apparently even years before patients got the vaccines[31]. The fact this confounding factor is overlooked demonstrates extreme confirmation bias and is the defining factor of Cargo Cult Science according to R.P. Feynman.[32]
(4) The Animal Models
Animal models reliably and repeatably show in RPC tests (a) that vaccines at the wrong time in development damage the adult brain or behavior [33][34] and (b) that multiple vaccines cause autoimmune disease even in animals bred to be non-autoimmune[35][36]. The effects are said to be robust, and as we’ve already seen there isn’t good human data rebutting them.
(5) The Contaminants
Studies have repeatedly found contaminants such as viruses, retroviruses, circoviruses, and human DNA in vaccines seemingly whenever tested,
and I’ve found no reason to believe off the shelf vaccines are free[37][38][39][40][41]. Reported contaminants have included SV-40 in polio vaccines which were administered even though scientists knew the vaccines were contaminated and already had hunches and experiments indicating SV-40 causes cancer[41][42]. Chimpanzee Coryza Virus became known in humans as RSV and has killed many millions of infants and hospitalizes 100,000/yr in America today[43]. Contaminated polio vaccine is plausibly also the origin of HIV[44][41]. There are discovered viral contaminants in vaccines today[38][39], with unknown long term effects, as well as I expect many undiscovered contaminants.
(6) Studies Ask Whether Some One Vaccine Damages, and Thus Miss That Many Do.
Virtually every study not reporting damage compares kids who got numerous vaccines to kids who got numerous vaccines. Such studies wouldn’t show statistically significant results no matter how much damage the vaccines are doing, unless one vaccine or vector by itself is doing comparable or more damage than the rest put together. The studies more or less test the hypothesis one vaccine is invisibly damaging, the rest are fine, and the studies are all obscured in the presence of multiple problems, much less the kind of timing and interaction effects observed in animal models. The one study[45] often touted as proving “The Risk of Autism is Not Increased by ‘Too Many Vaccines Too Soon’”[46] in fact compares patients based on antigens, and since DTP had more than 3000 antigens and no other vaccine common among the study patients had more than a handful, effectively compared patients who’d had DTP and dozens of vaccines to patients who did not have DTP (many had DTaP instead) and dozens of vaccines. The only counterexamples to this I’ve found are contrived in bizarre ways to avoid reality, such as the study that withheld the 2 month vaccines till 3 months from a group of kids, and asked the mothers, who were terrified enough a bunch insisted on changing back to the early vaccination group, to record symptoms with no doctor even consulted, identifying the placebo effect as vaccine prevention of diseases. The authors wrote it would have been unethical to give a placebo at 2 months to the kids getting the vaccine at 3 months, in order to do the experiment blind, but apparently consider it ethical to inject dozens of vaccines into your kids with zero placebo controlled testing.[47] [48]
(7) The Extensive Evidence Indicating Flu Vaccines Damage Immune Systems, Particularly in Children.
(8) The Epidemiological Studies That Aren’t Blatantly Confounded
All the credible ecological or epidemiological studies comparing people who got more vaccines to less indicate damage. For example,
Every empirical study I’ve read with a methodology that’s not clearly confounded consistently indicates vaccine damage.
(9) The Consistent Anecdotal and Informal Reports
Anecdotal and informal reports actually compare vaccinated and unvaccinated, unlike the contrived and confounded studies offered to support safety.
(10) The Authorities, Big Pharma, and Media Are Demonstrably Not Trustworthy.
To summarize 10 points in two: (A) the safety literature, wherever it doesn’t outright show vaccine damage, demonstrably is bollixed to where it doesn’t show much of anything. (B) Lots of peer reviewed publications cogently report lots of consistent damage that no published evidence rationally opposes, but are ignored by authorities and media.
The vaccine safety literature is laid out in considerable detail on this TruthSift diagram http://truthsift.com/search_view?topic=Are-Vaccines-Safe-?&id=406&nid=4083 where readers are invited to add more pertinent citations or arguments. Anybody who thinks I am confused on any point is invited to challenge any claim above and explain why[69]. Please feel free to ask your Pediatrician or other authority, and let me know what they say. I’ve submitted to 2 medical journals so far, but been unable to obtain a substantive review, a review citing any papers or making a case I’m wrong. As I receive no substantive rebuttal, it reaffirms what I have already concluded from extensive research, none exists.
If you’ve read the above, and are thinking: “you were right, I was deluded,” the next step is to ask yourself what else you may be deluded about, and what you can do about it. https://truthsift.com was designed to answer those questions.
If you think this post contains information that should be more widely known please share it.
References
[1] Adverse Effects of Vaccines: Evidence and Causality, Kathleen Stratton, Andrew Ford, Erin Rusch, and Ellen Wright Clayton, Editors; Committee to Review Adverse Effects of Vaccines; Institute of Medicine, The National Academies press 2011. 862pp.http://www.commed.vcu.edu/IntroPH/Communicable_Disease/2012/adverseffectsVaccines.pdf
[2] Immunization Safety Review: Multiple Immunizations and Immune Dysfunction Kathleen Stratton, Christopher B. Wilson and Marie C. McCormick, Editors, Immunization Safety Review Committee, Board on Health Promotion and Disease Prevention http://www.nap.edu/catalog/10306.html ISBN: 0−309−50866−5, 152 pages, 6 x 9, (2002) Institute of Medicine.
[3] Immunization Safety Review: Vaccines and Autism, Immunization Safety Review Committee, Institute of Medicine of the National Academies ISBN: 0−309−53275−2, 214 pages, 6 x 9, (2004) http://www.nap.edu/catalog/10997.html
[4] The Childhood Immunization Schedule and Safety: Stakeholder Concerns, Scientific Evidence, and Future Studies, Committee on the Assessment of Studies of Health Outcomes Related to the Recommended Childhood Immunization Schedule; Board on Population Health and Public Health Practice; Institute of Medicine ISBN 978−0−309−26702−1 230 pages (2013) http://www.nationalacademies.org/hmd/~/media/files/report%20files/2013/childhood-immunization-schedule/childhoodimmunizationscheduleandsafety_rb.pdf
[5] Conference report Workshop summary Aluminum in vaccines Vaccine 20 (2002) S1–S4 http://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0CCoQFjAA&url=http%3A%2F%2Farchive.hhs.gov%2Fnvpo%2Fnvac%2Fdocuments%2FAluminumws.pdf&ei=nZQoU5eIIoX0oAT5pYGgCg&usg=AFQjCNG_Zx126W2-nIJIMyTvE9LZz47V1g&sig2=c8Nu9WKzK27SBfJENfQXMw&bvm=bv.62922401
[6] Neonatal and early life vaccinology. Siegrist CA. Vaccine. 2001 May 14;19(25-26):3331-46. http://www.ncbi.nlm.nih.gov/pubmed/11348697
[7] Infants’ exposure to aluminum from vaccines and breast milk during the first 6 months, Dórea JG, Marques RC, Journal of Exposure Science and Environmental Epidemiology Volume 20, Issue 7, November 2010, Pages 598-601 http://www.ncbi.nlm.nih.gov/pubmed/20010978
[8] Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? Tomljenovic L, Shaw CA. J Inorg Biochem. 2011 Nov;105(11):1489-99 http://omsj.org/reports/tomljenovic%202011.pdf
[9] http://truthsift.com/search_view?topic=Are-Vaccines-Safe-?&id=406&nid=4083 See statement views for discussion and further citations
[10] Aluminum Neurotoxicity in Preterm Infants Receiving Intravenous-Feeding Solutions, Nicholas J. Bishop, M.D., Ruth Morley, M.B., B.Chir., J. Philip Day, Ph.D., and Alan Lucas, M.D. N Engl J Med 1997; 336:1557-1562May 29, 1997DOI: 10.1056/NEJM199705293362203 http://www.nejm.org/doi/full/10.1056/NEJM199705293362203#t=articleResults
[11] Aluminum exposure from parenteral nutrition in preterm infants: bone health at 15-year follow-up. Fewtrell MS, Bishop NJ, Edmonds CJ, Isaacs EB, Lucas A. http://www.ncbi.nlm.nih.gov/pubmed/19858156 Pediatrics. 2009 Nov;124(5):1372-9. doi: 10.1542/peds.2009-0783. Epub 2009 Oct 26. Erratum in Pediatrics. 2009 Dec;124(6):1709.
[12] http://truthsift.com/search_view?statement=Animal-Studies-report-results-tending-to-indicate-the-aluminum-is-toxic-in-the-quantities-administered-&id=406&nid=4133 See statement views for discussion and further citations
[13] Administration of aluminum to neonatal mice in vaccine-relevant amounts is associated with adverse long term neurological outcomes, C.A. Shaw, Y. Li , L. Tomljenovic, Journal of Inorganic Biochemistry, V 128, November 2013, Pages 237–244 http://www.sciencedirect.com/science/article/pii/S0162013413001773
[14] Slow CCL2-dependent translocation of biopersistent particles from muscle to brain, Zakir Khan, Christophe Combadière, François-Jérôme Authier, Valérie Itier, François Lux, Christopher Exley, Meriem Mahrouf-Yorgov, Xavier Decrouy, Philippe Moretto, Olivier Tillement, Romain K Gherardi BMC Medicine 201311:99 DOI: 10.1186÷1741−7015−11−99 http://bmcmedicine.biomedcentral.com/articles/10.1186/1741-7015-11-99
[15] http://truthsift.com/search_view?topic=Are-Vaccines-Safe-?&id=406 For discussion of other confirmatory citations
[16] Examination of the safety of pediatric vaccine schedules in a non-human primate model: assessments of neurodevelopment, learning, and social behavior. Curtis B, Liberato N, Rulien M, et al. 2015. Environ Health Perspect 123:579–589; http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4455585/
[18] Infant mortality rates regressed against number of vaccine doses routinely given: is there a biochemical or synergistic toxicity? Miller NZ, Goldman GS, Hum Exp Toxicol. 2011 Sep;30(9):1420-8. doi: 10.1177÷0960327111407644. Pub 2011 May 4. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3170075/
[19] A positive association found between autism prevalence and childhood vaccination uptake across the U.S. population. Delong G. J Toxicol Environ Health A. 2011;74(14):903-16. http://www.ncbi.nlm.nih.gov/pubmed/21623535
[20] Routine vaccinations and child survival: follow up study in Guinea-Bissau, West Africa Commentary: an unexpected finding that needs confirmation or rejection, Ines Kristensen, Peter Aaby, Henrik Jensen, BMJ 2000; 321 dos: http://dx.doi.org/10.1136/bmj.321.7274.1435
[21] Oral polio vaccination and low case fatality at the paediatric ward in Bissau, Guinea-Bissau. Aaby P, Rodrigues A, Biai S, et al ‚Vaccine. 2004 Aug 13;22(23-24):3014-7. http://www.ncbi.nlm.nih.gov/pubmed/15297050
[22] http://truthsift.com/search_view?id=406&nid=4144 See for further discussion and citations
[23] Special Issue ASIA – Autoimmune Syndrome Induced by Adjuvants, Lupus February 2012; 21 (2) http://lup.sagepub.com/content/21/2.toc
[24] Biopersistence and brain translocation of aluminum adjuvants of vaccines Front. Neurol., 05 February 2015 |http://dx.doi.org/10.3389/fneur.2015.00004
http://journal.frontiersin.org/article/10.3389/fneur.2015.00004/full
[25] Chronic fatigue syndrome and fibromyalgia following immunization with the hepatitis B vaccine: another angle of the ‘autoimmune (auto-inflammatory) syndrome induced by adjuvants’ (ASIA). Agmon-Levin N1, Zafrir Y, Kivity S, Balofsky A, Amital H, Shoenfeld Y. Immunol Res. 2014 Dec;60(2–3):376–83. doi: 10.1007/s12026-014‑8604-2.
[26] Study Reports Aluminum in Vaccines Poses Extremely Low Risk to Infants (2015−2016) http://www.fda.gov/BiologicsBloodVaccines/ScienceResearch/ucm284520.htm
[27] Updated aluminum pharmacokinetics following infant exposures through diet and vaccination, Mitkus RJ, King DB, Hess MA, Forshee RA, Walderhaug MO., Vaccine 29(51) 9538-43 2011. http://www.ncbi.nlm.nih.gov/pubmed/22001122
[28] Thimerosal Exposure in Infants and Developmental Disorders: A Retrospective Cohort Study in the United Kingdom Does Not Support a Causal Association, Nick Andrews; Elizabeth Miller; Andrew Grant et al, Pediatrics September 2004, VOLUME 114 / ISSUE 3 http://pediatrics.aappublications.org/content/114/3/584.full-text.pdf
[29] Prenatal and Infant Exposure to Thimerosal From Vaccines and Immunoglobulins and Risk of Autism, Cristofer S. Price, William W. Thompson, Barbara Goodson,et al, Pediatrics October 2010, VOLUME 126 / ISSUE 4 http://pediatrics.aappublications.org/content/126/4/656
[30] Autism Occurrence by MMR Vaccine Status Among US Children With Older Siblings With and Without Autism, Anjali Jain; Jaclyn Marshall; Ami Buikema; et al. JAMA. 2015;313(15):1534-1540. doi:10.1001/jama.2015.3077. http://jama.jamanetwork.com/article.aspx?articleid=2275444
[31] Transient suppression of atopy in early childhood is associated with high vaccination coverage, Gruber, C., S. Illi, S. Lau, R. Nickel, J. Forster, W. Kamin, C.P. Bauer, V. Wahn, U. Wahn, and the MAS-90 Study Group. 2003. . Pediatrics 111(3):e282-e288. http://pediatrics.aappublications.org/content/111/3/e282
[32] CARGO CULT SCIENCE (adapted from Caltech Commencement Address 1974), Richard P Feynman https://www.lhup.edu/~DSIMANEK/cargocul.htm
[33] Peripheral immune challenge with viral mimic during early postnatal period robustly enhances anxiety-like behavior in young adult rats.
Konat GW, Lally BE, Toth AA, Salm AK.Metab Brain Dis. 2011 Sep;26(3):237-40. doi: 10.1007/s11011-011-9244-z http://www.ncbi.nlm.nih.gov/pubmed/21643765
[34] Postnatal Inflammation Increases Seizure Susceptibility in Adult Rats, Michael A. Galic, Kiarash Riazi, James G. Heida, et al, The Journal of Neuroscience, 2 July 2008, 28(27): 6904-6913; doi: 10.1523/JNEUROSCI.1901-08.2008 http://www.jneurosci.org/content/28/27/6904.full
[35] Vaccine model of antiphospholipid syndrome induced by tetanus vaccine, L Dimitrijevi, I ivkovi, M Stojanovi, V Petrui, S ivanevi-Simonovi dos: 10.1177÷0961203311429816 Lupus February 2012 vol. 21 no. 2 195-202 http://lup.sagepub.com/content/21/2/195.abstract
[36] Self-Organized Criticality Theory of Autoimmunity, Ken Tsumiyama, Yumi Miyazaki, Shunichi Shiozawa 2009 DOI: 10.1371/journal.pone.0008382
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0008382
[37] Some oral poliovirus vaccines were contaminated with infectious SV40 after 1961. Cutrone R, Lednicky J, Dunn G, et al. Cancer Res. 2005 Nov
15;65(22):10273-9. http://www.ncbi.nlm.nih.gov/pubmed/16288015
[38] Viral Nucleic Acids in Live-Attenuated Vaccines: Detection of Minority Variants and an Adventitious Virus, J. G. Victoria, C. Wang, M. S. Jones,et al. J. Virol. June 2010 vol. 84 no. 12 6033-6040 http://jvi.asm.org/content/84/12/6033
[39] Viruses and Virus Nucleic Acid Contaminate Many Vaccines: Risks of cancer and creation of new pathogens should not be underplayed by regulators Prof. Joe Cummins http://www.i-sis.org.uk/Viruses_and_Virus_Nucleic_Acid_Contaminate_Vaccines.php
[40] Impact of environmental factors on the prevalence of autistic disorder after 1979, Theresa A. Deisher, Ngoc V. Doan, Angelica Omaiye, et al. Journal of Public Health and Epidemiology Vol. 6(9), pp. 271-284, 2014 DOI: 10.5897/JPHE2014.0649 http://soundchoice.org/scpiJournalPubHealthEpidem092014.pdf
[41] https://www.youtube.com/watch?v=13QiSV_lrDQ Dr. Maurice Hillman, The Merck Chief Scientist, discusses how the polio vaccine was administered although they knew it was contaminated with SV-40, which they strongly believed caused cancer. According to the tape, the monkeys from which the vaccine was being grown, were being kept in epidemic conditions crowded into cages, so they were all sick with a variety of viruses which then contaminated the vaccine stock. As Hillman discusses, SIV could very well have entered the human population this way as well.
[42] Association between simian virus 40 and non-Hodgkin lymphoma. Vilchez RA, Madden CR, Kozinetz CA, et al. Lancet. 2002 Mar 9;359(9309):817-23. http://www.ncbi.nlm.nih.gov/pubmed/11897278
[43] Polio eradication: a complex end game, Viera Scheibner, BMJ 2012;344:e2398 http://www.bmj.com/content/344/bmj.e2398/rapid-responses
[44] Polio vaccines and the origin of AIDS: some key writings, http://www.uow.edu.au/~bmartin/dissent/documents/AIDS/
[45] Increasing Exposure to Antibody-Stimulating Proteins and Polysaccharides in Vaccines Is Not Associated with Risk of Autism, Frank DeStefano, MD,MPH, Cristofer S. Price, ScM, Eric S. Weintraub, MPH DOI: http://dx.doi.org/10.1016/j.jpeds.2013.02.001
[46] The Risk of Autism is Not Increased by “Too Many Vaccines Too Soon”, Editorial of The Journal of Pediatrics http://www.jpeds.com/content/JPEDSDeStefano
[47] General Non-specific Morbidity is Reduced After Vaccination Within the Third Month of Life – the Greifswald Study, S. Otto, B. Mahner, I. Kadow, J. F. Beck, S. K.W. Wiersbitzky and R. Bruns, Journal of Infection (2000) 41, 172–175 doi: 10.1053/jinf.2000.0718, available online at http://www.idealibrary.com
[48] http://truthsift.com/node_info?nid=5340&superNode=No&subNode=No&isFlagged=No&probability=1&likelihoodEstimateT=0.5&likelihoodEstimateF=0.5&likelihoodEstimate=0.5&rating=TE
[49] Increased risk of noninfluenza respiratory virus infections associated with receipt of inactivated influenza vaccine. Cowling BJ, Fang VJ, Nishiura H, Chan KH, Ng S, Ip DK, Chiu SS, Leung GM, Peiris JS. Clin Infect Dis. 2012 Jun;54(12):1778-83. doi: 10.1093/cid/cis307. Epub 2012 Mar 15. http://www.ncbi.nlm.nih.gov/pubmed/22423139
[50] Effectiveness of trivalent inactivated influenza vaccine in influenza-related hospitalization in children: a case-control study. Joshi AY, Iyer VN, Hartz MF, Patel AM, Li JT. Allergy Asthma Proc. 2012 Mar-Apr;33(2):e23-7. doi: 10.2500/aap.2012.33.3513. http://www.ncbi.nlm.nih.gov/pubmed/22525386
[51] Association between the 2008-09 Seasonal Influenza Vaccine and Pandemic H1N1 Illness during Spring–Summer 2009: Four Observational Studies from Canada, Danuta M. Skowronski , Gaston De Serres, Natasha S. Crowcroft, et al.PLOS(2010), http://dx.doi.org/10.1371/journal.pmed.1000258
[52] Vaccination with whole inactivated virus vaccine affects the induction of heterosubtypic immunity against influenza virus A/H5N1 and immunodominance of virus-specific CD8+ T-cell responses in mice. Bodewes R, Kreijtz JH, Hillaire ML, Geelhoed-Mieras MM, Fouchier RA, Osterhaus AD, Rimmelzwaan GF. , J Gen Virol. 2010 Jul;91(Pt 7):1743-53. doi: 10.1099/vir.0.020784-0. Epub 2010 Mar 24. http://www.ncbi.nlm.nih.gov/pubmed/20335492
[53] Vaccination against human influenza A/H3N2 virus prevents the induction of heterosubtypic immunity against lethal infection with avian influenza A/H5N1 virus. Bodewes R, Kreijtz JH, Baas C, Geelhoed-Mieras MM, de Mutsert G, van Amerongen G, van den Brand JM, Fouchier RA, Osterhaus AD, Rimmelzwaan GF. PLoS One. 2009;4(5):e5538. doi: 10.1371/journal.pone.0005538. Epub 2009 May14. http://www.ncbi.nlm.nih.gov/pubmed/19440239
[54] Annual vaccination against influenza virus hampers development of virus-specific CD8+ T cell immunity in children. Bodewes R, Fraaij PL, Geelhoed-Mieras MM, van Baalen CA, Tiddens HA, van Rossum AM, van der Klis FR, Fouchier RA, Osterhaus AD, Rimmelzwaan GF., J Virol. 2011 Nov;85(22):11995-2000. doi: 10.1128/JVI.05213-11.Epub 2011 Aug 31. http://www.ncbi.nlm.nih.gov/pubmed/21880755
[55] Difference in immune response in vaccinated and unvaccinated Swedish individuals after the 2009 influenza pandemic, Isabelle Magalhaes Mikael Eriksson, Charlotte Linde, Rashid Muhammad, Lalit Rane, Aditya Ambati, Rebecca Axelsson-Robertson, Bahareh Khalaj, Nancy Alvarez-Corrales, Giulia Lapini, Emanuele Montomoli, Annika Linde, Nancy L Pedersen,3 and Markus Maeurer BMC Infect Dis. 2014; 14: 319.Published online 2014 Jun 11. doi: 10.1186÷1471−2334−14−319 PMCID: PMC4067073 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4067073/
[56] “Vaccine effectiveness was estimated as 100% x (1 — odds ratio [ratio of odds of being vaccinated among outpatients with influenza-positive test results to the odds of being vaccinated among outpatients with influenza-negative test results])”, Center for Disease Control, Early Estimates of Seasonal Influenza Vaccine Effectiveness — United States, January 2015 Weekly January 16, 2015 / 64(01);10-15 http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6401a4.htm
[57] http://truthsift.com/node_info?nid=2823&superNode=No&subNode=No&isFlagged=No&probability=1&likelihoodEstimateT=0.5&likelihoodEstimateF=0.5&likelihoodEstimate=0.5&rating=TE for more discussion
[58] Combining Childhood Vaccines at One Visit Is Not Safe, Neil Z. Miller, Journal of American Physicians and Surgeons Volume 21 Number 2 Summer 2016 http://www.jpands.org/vol21no2/miller.pdf
[59] Adverse events following HPV vaccination, Alberta 2006–2014, Xianfang C. Liu, , Christopher A. Bell, , Kimberley A. Simmonds, , Lawrence W. Svensona, Margaret L. Russell, Vaccine Volume 34, Issue 15, 4 April 2016, Pages 1800–1805 http://www.sciencedirect.com/science/article/pii/S0264410X16002036
[60] For further data analysis and discussion see http://truthsift.com/node_info?nid=5196&superNode=No&subNode=No&isFlagged=No&probability=1&likelihoodEstimateT=0.5&likelihoodEstimateF=0.5&likelihoodEstimate=0.5&rating=TE
[61] http://www.vaccinationcouncil.org/2009/05/22/a-pretty-big-secret/
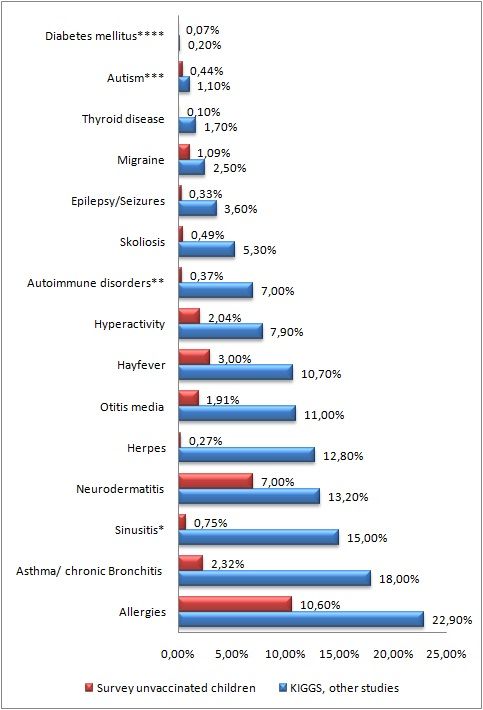
[62] http://www.vaccineinjury.info/survey/results-unvaccinated/results-illnesses.html
[63] https://www.youtube.com/results?search_query=%23hearthiswell
[64] http://www.morganverkamp.com/august-27-2014-press-release-statement-of-william-w-thompson-ph-d-regarding-the-2004-article-examining-the-possibility-of-a-relationship-between-mmr-vaccine-and-autism/
[65] https://sharylattkisson.com/cdc-scientist-we-scheduled-meeting-to-destroy-vaccine-autism-study-documents/
[66] http://projects.propublica.org/graphics/bigpharma
[67] http://www.washingtonsblog.com/2015/06/editors-in-chief-of-worlds-most-prestigious-medical-journals-much-of-the-scientific-literature-perhaps-half-may-simply-be-untrue-it-is-simply-no-longer-poss.html
[68] http://www.nybooks.com/articles/2009/01/15/drug-companies-doctorsa-story-of-corruption/
[69] http://truthsift.com/search_view?topic=Are-Vaccines-Safe-?&id=406

Fox 29 — Good Day Philadelphia
http://www.fox29.com/140735577-video
NBC TV 10
CNN en Espanol
http://cnnespanol.cnn.com/video/cnnee-encuentro-intvw-joel-osorio-bioquantina-muerte-cerebral/

Bioquark, Inc., (http://www.bioquark.com) a company focused on the development of novel biologics for complex regeneration and disease reversion, and Revita Life Sciences, (http://revitalife.co.in) a biotechnology company focused on translational therapeutic applications of autologous stem cells, have announced that they have received IRB approval for a study focusing on a novel combinatorial approach to clinical intervention in the state of brain death in humans.
This first trial, within the portfolio of Bioquark’s Reanima Project (http://www.reanima.tech) is entitled “Non-randomized, Open-labeled, Interventional, Single Group, Proof of Concept Study With Multi-modality Approach in Cases of Brain Death Due to Traumatic Brain Injury Having Diffuse Axonal Injury” (https://clinicaltrials.gov/ct2/show/NCT02742857?term=bioquark&rank=1), will enroll an initial 20 subjects, and be conducted at Anupam Hospital in Rudrapur, Uttarakhand India.
“We are very excited about the approval of our protocol,” said Ira S. Pastor, CEO, Bioquark Inc. “With the convergence of the disciplines of regenerative biology, cognitive neuroscience, and clinical resuscitation, we are poised to delve into an area of scientific understanding previously inaccessible with existing technologies.”
Death is defined as the termination of all biological functions that sustain a living organism. Brain death, the complete and irreversible loss of brain function (including involuntary activity necessary to sustain life) as defined in the 1968 report of the Ad Hoc Committee of the Harvard Medical School, is the legal definition of human death in most countries around the world. Either directly through trauma, or indirectly through secondary disease indications, brain death is the final pathological state that over 60 million people globally transfer through each year.
While human beings lack substantial regenerative capabilities in the CNS, many non-human species, such as amphibians, planarians, and certain fish, can repair, regenerate and remodel substantial portions of their brain and brain stem even after critical life-threatening trauma.

Additionally, recent studies on complex brain regeneration in these organisms, have highlighted unique findings in relation to the storage of memories following destruction of the entire brain, which may have wide ranging implications for our understanding of consciousness and the stability of memory persistence.
“Through our study, we will gain unique insights into the state of human brain death, which will have important connections to future therapeutic development for other severe disorders of consciousness, such as coma, and the vegetative and minimally conscious states, as well as a range of degenerative CNS conditions, including Alzheimer’s and Parkinson’s disease,” said Dr. Sergei Paylian, Founder, President, and Chief Science Officer of Bioquark Inc.
Over the years, clinical science has focused heavily on preventing such life and death transitions and made some initial progress with suspended animation technologies, such as therapeutic hypothermia. However, once humans transition through the brain death window, currently defined by the medical establishment as “irreversible”, they are technically no longer alive, despite the fact that human bodies can still circulate blood, digest food, excrete waste, balance hormones, grow, sexually mature, heal wounds, spike a fever, and gestate and deliver a baby. It is even acknowledged by thought leaders that recently brain dead humans still may have residual blood flow and electrical nests of activity in their brains, just not enough to allow for an integrated functioning of the organism as a whole.
“We look forward to working closely with Bioquark Inc. on this cutting edge clinical initiative,” said Dr. Himanshu Bansal, Managing Director of Revita Life Sciences.
About Bioquark, Inc.
Bioquark Inc. is focused on the development of natural biologic based products, services, and technologies, with the goal of curing a wide range of diseases, as well as effecting complex regeneration. Bioquark is developing both biological pharmaceutical candidates, as well as products for the global consumer health and wellness market segments.
About Revita Life Sciences
Revita Life Sciences is a biotechnology company focused on the development of stem cell therapies that target areas of significant unmet medical need. Revita is led by Dr. Himanshu Bansal MD, PhD. who has spent over two decades developing novel MRI based classifications of spinal cord injuries as well as comprehensive treatment protocols with autologous tissues including bone marrow stem cells, dural nerve grafts, nasal olfactory tissues, and omental transposition.

I have spent the last 30 years in various aspects of the biopharmaceutical industry, which for the most part has been a very rewarding experience.
However, during this time period, having been immersed many different components of therapeutic development and commercialization, one thing has always bothered me: a wide array of promising research never makes it off the bench to see the translational light of day, and gets lost in the historical scientific archives.
I always believed that scientific progress happened in a very linear narrative, with each new discovery supporting the next, resulting ultimately in an eventual stairway of scientific enlightenment.
What the reality turned out to be was much more of a fragmented, research “evolutionary tree”, with dozens of potential pathways, only very few branches of which ever resulted in scientific maturity, and not always the most fruitful ones by any means.
The premature extinction of these promising discovery pathways were the result of a variety of factors, including, but not limited to, funding priorities, competing industrial interests, “out of vogue” concepts, lack of intellectual properties, non-existent regulatory models, conflicted legislative initiatives, and even religious implications.
In 2016, as in previous years, we continue to see these “valleys of death” swallow up pathways of scientific possibility, with few popular segments attracting the majority of attention and support.

The preponderance of resources focused on the somatic mutation model of carcinogenesis, despite an endless range of research highlighting that the disease is extremely heterogenic and rarely ever follows such a clonal model, is one example that continues to be inappropriately manifested in the oncology system, decades into the “war on cancer”.
On a similar plane, the jettisoning of most studies of the biophysical aspects of human genetics, despite the gross incompleteness offered by the central dogma to explain higher biological form and function, is another example that has become all too pervasive in the research community.
And then there are the areas of human consciousness, memory, and information processing / storage, where in many ways we are still operating in the dark ages, with materialists and dualists battling it out for centuries.
One topic that I have written quite a bit about is that of death, specifically that of the death of the human brain — http://www.singularityweblog.com/is-death-reversible/
While I am a staunch supporter and advocate of the life-extension / anti-aging movement, I am equally vocal about our need to develop technologies, products, and services that can actually reverse our ultimate transition between the living and dead states, a transition that occurs annually for 60 million humans around the globe.
Death, however, is unfortunately seen by many as a natural, biological progression for human beings, and in many circles, deemed an unnecessary area of scientific research and exploration.
I beg to differ.
Far too often, death arrives too early and too unexpectedly for many of us and our loved ones. And the best modern medicine has to offer today is “Sorry. There is nothing else we can do.”
But what if there was?
There are a variety of species across the natural world that are capable of regenerating and repairing themselves from forms of severe CNS damage that bring them to the transitional grey zone between life and death. Along the evolutionary timeline however, this ability gradually disappeared hundreds of millions of years ago and does not manifest in higher species.

Now, in the 21st century, with the convergence of the disciplines of regenerative biology, cognitive neuroscience, and clinical resuscitation, we may finally be poised to take back these capabilities for humans.
Over the years, clinical science has focused heavily on preventing such life and death transitions and made some initial progress with suspended animation technologies, such as therapeutic hypothermia. But once we transition through the brain death window, currently defined by the medical establishment as “irreversible” (per the 1968 Ad Hoc Committee of the Harvard Medical School definition), we are technically no longer alive.

To add insult to injury, a human can be declared dead, even while our bodies can still circulate blood, digest food, excrete waste, balance hormones, grow, sexually mature, heal wounds, spike a fever, and gestate and deliver a baby. It is even acknowledged by thought leaders that recently brain dead humans still may have residual blood flow and electrical nests of activity in their brains, just not enough to allow for an integrated functioning of the organism as a whole.
Several prominent cases in the media over the past few years have further served to highlight the current situation, as well as the substantial anatomical and functional differences between the state known as brain death, and other severe disorders of consciousness, such as coma, and the vegetative and minimally conscious states.
It is now time to take the necessary steps to provide new possibilities of hope, in order to counter the pain, sorrow, and grief that is all too pervasive in the world when we experience a loved one’s unexpected or untimely death, due to lesions which might be potentially reversible with the application of promising neuro-regeneration and neuro-reanimation technologies and therapies.

It is time to undertake the required research, based on 2016 technological knowledge, in order to bring about such transformational change.
My name is Ira S. Pastor and I am the CEO of the biotechnology company Bioquark Inc.
Welcome to the unveiling of the Reanima project.
OK. In scientific terms, it is only a ‘hypothesis’ — the reverse of the ‘Disposable Soma’ theory of ageing. Here how it goes.
For the past several decades, the Disposable Soma theory of ageing has been enjoying good publicity and a lively interest from both academics and the public alike. It stands up to scientific scrutiny, makes conceptual sense and fits well within an evolutionary framework of ageing. The theory basically suggests that, due to energy resource constraints, there is a trade-off between somatic cell and germ cell repair. As a result, germ cells are being repaired effectively and so the survival of the species is assured, at a cost of individual somatic (bodily) ageing and death. To put it very simply, we are disposable, we age and die because all the effective repair mechanisms have been diverted to our germ cell DNA in order to guarantee the survival of our species.
The theory accounts for many repair pathways and mechanisms converging upon the germ cell, and also for many of those mechanisms being driven away from somatic cell repair just to ensure germ cell survival. In the past two or three years however, it is increasingly being realised that this process is not unidirectional (from soma to germ), but it is bi-directional: under certain circumstances, somatic cells may initiate damage that affects germ cells, and also that germ cells may initiate repairs that benefit somatic cells!
I can’t even begin to describe how important this bi-directionality is. Taking this in a wider and more speculative sense, it is, in fact, the basis for the cure of ageing. The discovery that germ cells can (or are forced to) relinquish their repair priorities, and that resources can then be re-allocated for somatic repairs instead, means that we may be able to avoid age-related damage (because this would be repaired with greater fidelity) and, at the same time, avoid overpopulation (as our now damaged genetic material would be unsuitable for reproduction).
Ermolaeva et al. raised the further possibility that DNA damage in germ cells may protect somatic cells. They suggested that DNA injury in germ cells upregulates stress resistance pathways in somatic cells, and improves stress response to heat or oxidation. This is profoundly important because it shows that, in principle, when germ cells are damaged, they produce agents which can then protect somatic cells against systemic stress.
This mechanism may reflect an innate tendency to reverse the trade-offs between germ cell and somatic cell repair: when the germ cells are compromised, there is delay in offspring production matched by an increased repair of somatic cells. In Nature’s ‘eyes’, if the species cannot survive, at least the individual bodies should.
In addition, it was shown that neuronal stress induces apoptosis (orderly cell death) in the germ line. This process is mediated by the IRE-1 factor, an endoplasmic reticulum stress response sensor, which then activates p53 and initiates the apoptotic cascade in the germ line. Therefore germ cells may die due to a stress response originating from the distantly-located neurons.
If this mechanism exists, it is likely that other similar mechanisms must also exist, waiting to described. The consequence could be that neuronal positive stress (i.e. exposure to meaningful information that entices us to act) can affect our longevity by downgrading the importance of germ cell repair in favour of somatic tissue repair. In other words, the disposable soma theory can be seen in reverse: the soma (body) is not necessarily disposable but it can survive longer if it becomes indispensable, if it is ‘useful to the whole. This, as we claimed last week, can happen through mechanisms which are independent of any artificial biotechnological interventions.
We know that certain events which downgrade reproduction, may also cause a lifespan extension. Ablation of germ cells in the C.elegans worm, leads to an increased lifespan, which shows that signals from the germline have a direct impact upon somatic cell survival, and this may be due to an increased resistance of somatic cells to stress. Somatic intracellular clearance systems are also up-regulated following signals from the germ line.
In addition, protein homoeostasis in somatic cells is well-maintained when germ cells are damaged, and it is significantly downgraded when germ cell function increases. All of the above suggest that when the germ cells are healthy, somatic repair decreases, and when they are not, somatic repair improves as a counter-effect.
In an intriguing paper published last month, Lin et al. showed that under certain circumstances, somatic cells may adopt germ-like characteristics, which may suggest that these somatic cells can also be subjected to germ line protection mechanisms after their transformation. A few days ago Bazley et al. published a paper elucidating the mechanisms of how germ cells may induce somatic cell reprogramming and somatic stem cell pluripotency. This is an additional piece of evidence of the cross-talk mechanisms between soma and germ line, underscoring the fact that the health of somatic tissues depends upon signals from the germ line.
In all, there is sufficient initial evidence to suggest that my line of thinking is quite possibly correct: that the disposable soma theory is not unidirectional and the body may not, after all, be always ‘disposable’. Under certain evolutionary pressures we could experience increased somatic maintenance at the expense of germ cell repairs, and thus reach a situation where the body actually lives longer. I have already discussed that some of these evolutionary pressures could be dependent upon how well one makes themselves ‘indispensable’ to the adaptability of the homo sapiens species within a global techno-cultural environment.